
The Patient-Centred Infrastructure Precision Medicine Has Been Waiting For

Author: Bahar Folad, Multi-omics Research Analyst, Axia Medicine
Published by Axia Medicine | November 2025
This is the fourth article of a series. Previous entries:
Precision medicine promises a paradigm shift in healthcare: earlier prevention, more confident diagnoses, and treatments tailored to an individual's genetic profile, environment and lifestyle. Yet, as we explored across the earlier articles, The Genomics Paradox, The Multimodal Shift and Precision Public Health, access to genomic technologies remains uneven, AI cannot deliver on hospital records alone and population-level insights break down whenever data is trapped within separate institutional silos. Together, these patterns reveal a deeper structural dilemma: our Real World Evidence systems continue to centre institutions rather than the patients whose data drives discovery.
Traditional clinical research illustrates this clearly. Barriers to entry, e.g., geographical distance from study sites, cost of travel and participation, insufficient awareness of clinical trials among eligible patients, restricted digital access, limited availability due to previous commitments, and cultural or linguistic mismatch, shape who participates. Only about 5% of eligible patients enrol in clinical trials, and up to 20% of trials terminate early due to recruitment shortfalls (Goodson et al., 2022).
The paradox is striking: as medicine becomes more personalised, the evidence base behind it continues to treat patients as interchangeable. Persistent and well-documented recruitment barriers systemically limit who can take part, yielding a consistently unrepresentative participant cohort (Collister, Song and Ruzycki, 2024; Anand et al., 2025; Pardhan et al., 2025). This lack of diversity undermines data generalisability and fragments scientific progress at the very moment broader insight is needed.
Emerging decentralised designs show that when trials are centred on the individual, participation expands and outcomes improve, strengthening the evidence base that precision medicine depends on.
Decentralised Clinical Trials: From Participation to Partnership
Decentralised Clinical Trials (DCTs) reconfigure trial activities around patients rather than research sites (Figure 1). Rather than participants having to travel repeatedly to hospitals or research centres for screening, consent, monitoring and sample collection, consent can occur digitally; visits shift to telemedicine; vital signs and symptoms are captured through wearable and remote sensors; mobile nurses collect samples in the home.
DCTs emerged in the early 2010s, with studies in the U.S. and U.K. assessing feasibility (Wang et al., 2025). Adoption accelerated during COVID-19; with patient mobility restricted, decentralisation moved from optional to essential. The U.S. issued early FDA guidance; Europe expanded hybrid approaches through EMA and national health systems, with several regulators such as Denmark and Sweden introducing DCT-specific frameworks beyond the pandemic (Vayena et al., 2023). As discussed in Precision Public Health, Covid-19 showed how systems fail when data stays locked inside institutions. DCTs apply the same individual-centred logic to research, enabling participation and visibility at a population scale.
Today, the industry is at an inflection point: DCTs are no longer a pandemic workaround but a rapidly evolving redesign of how research reaches people. In 2024, the DCT market surpassed USD 9 billion and is projected to exceed USD 38 billion by 2034, reflecting a fundamental change in how trials are delivered. Today’s DCT ecosystem spans contract research organisations (CROs), clinical sites adapting to hybrid models; pharmaceutical sponsors adopting decentralised protocols; technology platforms enabling eConsent and wearables integration; and home-health providers. Decentralisation has become an integrated industry rather than a methodological footnote.
Singapore’s PROMOTE trial demonstrated what a fully decentralised randomised design can achieve: a 97% retention rate, reporting higher patient convenience and reduced environmental impact relative to traditional designs (Fries et al., 2025). Broader analyses confirm these benefits: DCTs improve geographical access, population diversity, and operational efficiency (Jean-Louis and Seixas, 2024). When supported by robust, standardised data protocols, decentralisation enhances representativeness and generalisability of evidence across diverse populations (Kelsey et al., 2023; de Jong et al., 2024).
Critically, DCT experience has shown a consistent pattern: when patients are engaged early in trial design, consent processes, and transparency around treatment requirements, trust improves (Sinha et al., 2024). In essence, decentralisation transforms the research interface: from a one-way transaction to a reciprocal partnership.
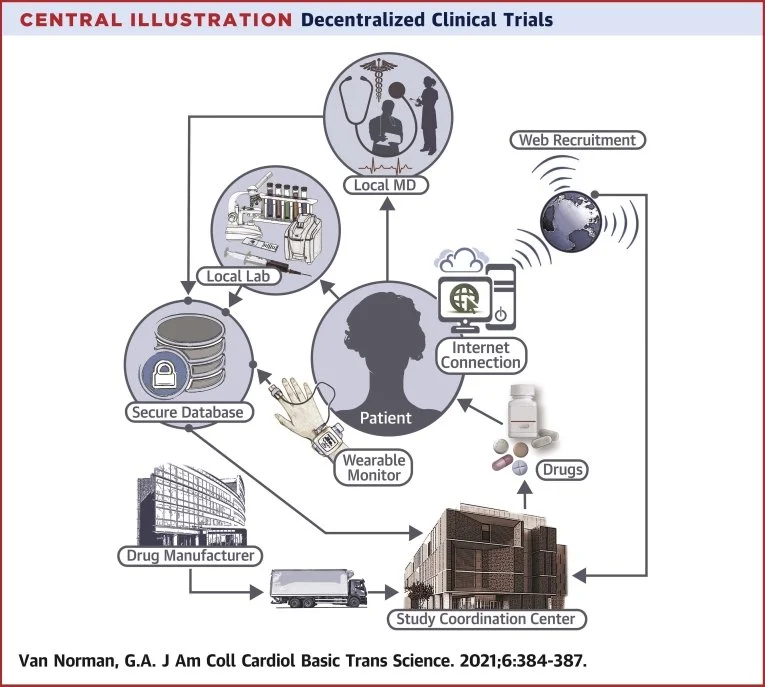
Figure 1. Schematic showing how DCTs centre participation around the patient through web-based recruitment, local clinicians and labs, secure data transmission and direct drug supply.
Source: Van Norman, G.A. (2021). Decentralized Clinical Trials. JACC: Basic to Translational Science, 6(4), 384–387.
The expansion of decentralised clinical approaches coincides with a broader shift toward multimodal health data. Contemporary clinical AI increasingly depends not only on electronic health records, but also on genomics, imaging, physiological signals, environmental exposures, and behavioural and patient-reported data to support robust and generalisable models of health. Multimodal AI systems consistently outperform unimodal approaches in diagnostic accuracy and resilience across clinical tasks.
Despite this potential, progress in multimodal AI remains uneven across specialties. This reflects structural features of healthcare delivery rather than limitations in clinical practice. Hospitals and clinics are designed to provide safe, accountable, episodic care and to anchor diagnosis and treatment within established governance frameworks. While essential, this model captures only fragments of the continuous physiological, behavioural, and environmental context through which conditions develop and change. As a result, current AI systems perform well on static diagnostic tasks but remain limited in supporting prognosis, disease progression, and prevention (Schouten et al., 2025).
Decentralised participation offers a complementary pathway. Automated data capture, remote monitoring, and continuous consent processes enable the generation of longitudinal, richly phenotyped datasets between clinical encounters, strengthening the evidentiary base for multimodal AI. Challenges around interpretability, workflow integration, privacy, and consent persist (Xu et al., 2024), but decentralised models bring data generation closer to patients’ lived experience in ways that can meaningfully support clinical understanding.
If multi-omics integration is the analytical engine of precision medicine, transparency and patient agency form its clinical interface. Only when individuals can understand and control how their data are used can participation be sustained and populations represented with sufficient depth and equity. Without this foundation of trust, multimodal AI cannot realise its clinical or public health potential.
Biomarker Discovery: Turning Multi-Omic Data into Meaning
Biomarker discovery is one of the clearest and most immediate benefits of multi-omics. When genomics, proteomics, transcriptomics, and metabolomics analyses are integrated, they reveal molecular signatures that single data types cannot capture. This approach has enabled unprecedented insights across cancer, cardiovascular and neurodegenerative disorders, and diabetes (Dar et al., 2023). Recent findings include endometrial cancer–specific biomarkers, (An et al., 2025) and tissue repair and regeneration biomarkers such as TGF-β, VEGF, IL-6, and multiple matrix metalloproteinases (MMPs) (Liu et al., 2025).
Trained on data from UK Biobank, the MILTON ensemble machine-learning framework predicted outcomes across more than 3,000 diseases, illustrating the power of integrating clinical biomarkers and phenotypes (Garg et al., 2024). But to reiterate The Multimodal Shift, UK Biobank is an exception: a national, centralised resource built over more than a decade. The limiting factor is not machine learning or multi-omics technology, but the absence of architecture capable of generating longitudinal and clinically-grounded datasets. Without that foundation, distributed multi-omic biobanks remain aspirational. When data moves with patients across settings, the scope and equity of biomarker discovery can expand dramatically.
From Data Mines to Data Stakeholders
Across decentralised trials, multimodal data, and multi-omics research, the same pattern emerges: reducing barriers increases diversity; longitudinal data reveals what single snapshots cannot; and transparency strengthens the trust necessary for sustained patient engagement.
Unlocking this potential requires infrastructure built for shared stewardship: continuous multimodal data collection with programmatic, consented access for researchers. When data moves with the patient rather than staying in silos, decentralised models can generate the diverse, dynamic evidence precision medicine needs. Clinicians gain the full picture of a patient’s health, not just episodic encounters or isolated results, enabling greater ethical oversight and continuity of care. Trial eligibility becomes visible within routine workflows, and collaboration with external investigators becomes simpler because data arrives with provenance, consistency and consent already in place.
In this model, patients are not sources of data to be mined, but active participants whose contributions shape discovery. Clinics are not data custodians working in isolation but key partners in a network of precision care and research. Building this patient-centered foundation is essentially for delivering the full promise of precision medicine: for patients, for care providers, and at population scale.
References
Akhloufi, M.A. and Janboudi, B. (2025). Multimodal Artificial Intelligence in Medical Diagnostics. Information, [online] 16(7), pp.591–591. doi:https://doi.org/10.3390/info16070591.
Anand, S.S., Bosch, J., Mehran, R., Mehta, S.R. and Patel, M.R. (2025). Designing inclusive clinical trials: how researchers can drive change to improve diversity. BMJ, pp.e082485–e082485. doi:https://doi.org/10.1136/bmj-2024-082485.
An, Y., Feng, Q., Jia, L., Sha, X., Zhang, T., Lu, L., Wang, R. and Bai, B. (2025). Present progress in biomarker discovery of endometrial cancer by multi-omics approaches. Clinical Proteomics, 22(1). doi:https://doi.org/10.1186/s12014-025-09528-6.
Collister, D., Song, C. and Ruzycki, S.M. (2024). Fostering diversity in clinical trials: need for evidence and implementation to improve representation. BMJ Medicine, 3(1), pp.e000984–e000984. doi:https://doi.org/10.1136/bmjmed-2024-000984.
Dar, M.A., Arafah, A., Bhat, K.A., Khan, A., Khan, M.S., Ali, A., Ahmad, S.M., Rashid, S.M. and Rehman, M.U. (2022). Multiomics technologies: role in disease biomarker discoveries and therapeutics. Briefings in Functional Genomics, 22(2). doi:https://doi.org/10.1093/bfgp/elac017.
de Jong, A.J., Shahid, N., Zuidgeest, M.G.P., Santa-Ana-Tellez, Y., Hogervorst, M., Goettsch, W., Traore, H., de Boer, A. and Gardarsdottir, H. (2024). Opportunities and Challenges for Decentralized Clinical Trial Approaches: European Health Technology Assessment Perspective. Value in Health, 27(3), pp.294–300. doi:https://doi.org/10.1016/j.jval.2023.11.006.
Fries, L.R., Khaled, N., Santos, I.V., Suniega-Tolentino, E., Motshewa Sesing, Melissa, Yang, C.Y., Chan, S.Y. and Mottaz, S.C. (2025). Decentralized clinical trials are better for the participants and for the planet: the case study of a double-blind randomized controlled trial in Singapore (PROMOTE study). Frontiers in Public Health, [online] 12. doi:https://doi.org/10.3389/fpubh.2024.1508166.
Garg, M., Karpinski, M., Matelska, D., Middleton, L., Burren, O.S., Hu, F., Wheeler, E., Smith, K.R., Fabre, M.A., Mitchell, J., O’Neill, A., Ashley, E.A., Harper, A.R., Wang, Q., Dhindsa, R.S., Petrovski, S. and Dimitrios Vitsios (2024). Disease prediction with multi-omics and biomarkers empowers case–control genetic discoveries in the UK Biobank. Nature Genetics, [online] 56(9), pp.1821–1831. doi:https://doi.org/10.1038/s41588-024-01898-1.
Goodson, N., Wicks, P., Morgan, J., Hashem, L., Callinan, S. and Reites, J. (2022). Opportunities and counterintuitive challenges for decentralized clinical trials to broaden participant inclusion. npj Digital Medicine, 5(1). doi:https://doi.org/10.1038/s41746-022-00603-y.
Kelsey, M.D., Patrick-Lake, B., Abdulai, R., Broedl, U.C., Brown, A., Cohn, E., Curtis, L.H., Komelasky, C., Mbagwu, M., Mensah, G.A., Mentz, R.J., Nyaku, A., Omokaro, S.O., Sewards, J., Whitlock, K., Zhang, X. and Bloomfield, G.S. (2022). Inclusion and diversity in clinical trials: Actionable steps to drive lasting change. Contemporary Clinical Trials, [online] 116(1), p.106740. doi:https://doi.org/10.1016/j.cct.2022.106740.
Krones, F., Marikkar, U., Parsons, G., Szmul, A. and Mahdi, A. (2024). Review of multimodal machine learning approaches in healthcare. [online] arXiv.org. Available at: https://arxiv.org/abs/2402.02460?utm_source=chatgpt.com [Accessed 17 Nov. 2025].
Lee, S.J. and Rho, M. (2022). Multimodal deep learning applied to classify healthy and disease states of human microbiome. Scientific Reports, 12(1). doi:https://doi.org/10.1038/s41598-022-04773-3.
Liu, J., Yang, L., Liu, D., Wu, Q., Yu, Y., Huang, X., Li, J. and Liu, S. (2025). The role of multi-omics in biomarker discovery, diagnosis, prognosis, and therapeutic monitoring of tissue repair and regeneration processes. Journal of Orthopaedic Translation, [online] 54, pp.131–151. doi:https://doi.org/10.1016/j.jot.2025.07.006.
Pardhan, S., Sehmbi, T., Wijewickrama, R., Onumajuru, H. and Piyasena, M.P. (2025). Barriers and facilitators for engaging underrepresented ethnic minority populations in healthcare research: an umbrella review. International journal for equity in health, [online] 24(1), p.70. doi:https://doi.org/10.1186/s12939-025-02431-4.
Schouten, D., Nicoletti, G., Dille, B., Chia, C., Vendittelli, P., Schuurmans, M., Litjens, G. and Khalili, N. (2024). Navigating the landscape of multimodal AI in medicine: a scoping review on technical challenges and clinical applications. [online] arXiv.org. Available at: https://arxiv.org/abs/2411.03782.
Seixas, A.A. and Jean-Louis, G. (2024). The value of decentralized clinical trials: Inclusion, accessibility, and innovation. Science, 385(6711). doi:https://doi.org/10.1126/science.adq4994.
Van Norman, G.A. (2021). Decentralized Clinical Trials. JACC: Basic to Translational Science, 6(4), pp.384–387. doi:https://doi.org/10.1016/j.jacbts.2021.01.011.
Vayena, E., Blasimme, A. and Sugarman, J. (2023). Decentralised clinical trials: ethical opportunities and challenges. The Lancet Digital Health, 5(6). doi:https://doi.org/10.1016/s2589-7500(23)00052-3.
Wang, H., Daizadeh, N., Shen, Y., Chen, J., Rockhold, F.W., Pang, H. and Lee, H. (2025). Decentralized Clinical Trials in the Era of Real‐World Evidence: A Critical Assessment of Recent Experiences. Clinical and Translational Science, [online] 18(9), pp.e70328–e70328. doi:https://doi.org/10.1111/cts.70328.
Xu, X., Li, J., Zhu, Z., Zhao, L., Wang, H., Song, C., Chen, Y., Zhao, Q., Yang, J. and Pei, Y. (2024). A Comprehensive Review on Synergy of Multi-Modal Data and AI Technologies in Medical Diagnosis. Bioengineering, [online] 11(3), pp.219–219. doi:https://doi.org/10.3390/bioengineering11030219.